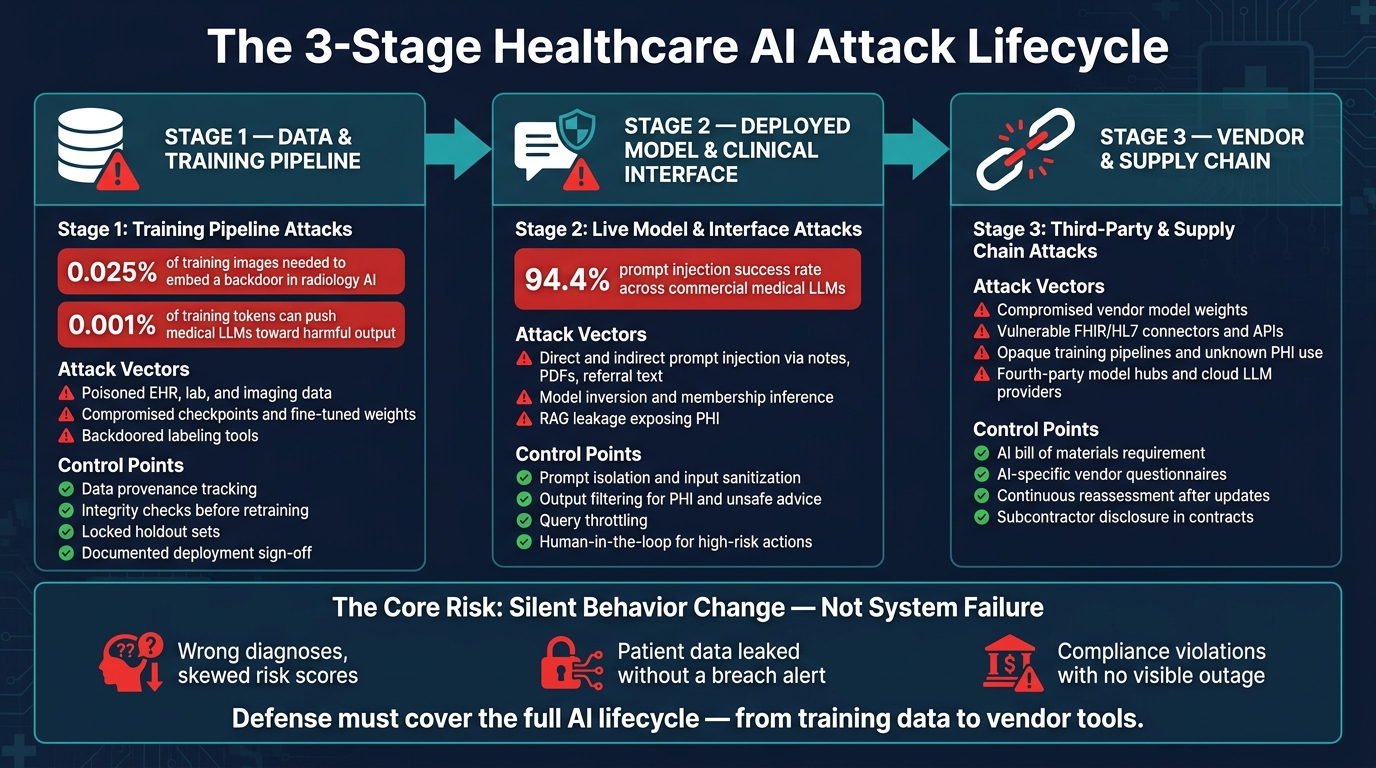
I see the main point like this: these attacks change model behavior across the full AI lifecycle - from training data, to live prompts, to vendor tools. In healthcare, that can mean bad recommendations, PHI exposure, and HIPAA risk without a clear system outage.
Here’s the article in plain English:
-
Stage 1: Training pipeline attacks
- Poisoned EHR, lab, or imaging data can shift model output before launch.
- A backdoor may need only 0.025% of training images.
- Even tiny changes in medical LLM training data - around 0.001% of tokens - can push harmful output.
-
Stage 2: Live model and interface attacks
- Prompt injection can steer clinical assistants through chat inputs, notes, PDFs, or referral text.
- One study found prompt injection worked in 94.4% of tests on medical LLMs.
- Query attacks can expose PHI through model inversion, membership inference, or RAG leakage.
- Stage 3: Vendor and supply chain attacks
What I’d take away: you need controls at each step - data lineage checks, model integrity checks, prompt and output filtering, query limits, human review for high-risk actions, and AI-specific vendor review.
| Stage | Main risk | What can go wrong |
|---|---|---|
| Training | Poisoned data or backdoored checkpoints | Wrong risk scores, bad diagnosis patterns |
| Deployment | Prompt injection and query abuse | Unsafe advice, hidden tool actions, PHI leaks |
| Supply chain | Compromised vendor components | Bad outputs or data exposure through outside tools |
If I had to sum it up in one line: healthcare AI risk is less about system failure and more about silent behavior change.
Healthcare AI Attack Lifecycle: 3 Stages of Risk & Key Controls
AI Cybersecurity Risks and Compliance for Healthcare Organizations
sbb-itb-535baee
Stage 1: Data and Training Pipeline Attacks
Stage 1 starts in the data pipeline. That’s where poisoned inputs can change model behavior before deployment.
Data Poisoning in EHR, Imaging, and Clinical Labeling Workflows
At this stage, the main danger is poisoned input. Most training security plans assume the data is clean. In healthcare, that assumption often falls apart. Training data moves through EHR exports, HL7/FHIR interfaces, imaging archives, labeling vendors, and federated learning nodes spread across multiple facilities.
An attacker who gets into an interface engine, or who takes over a clinician account, could quietly change lab values like troponin, creatinine, or D-dimer within a clinically plausible range. On paper, the numbers still look normal enough. But the model may start to underestimate risk for a certain patient group, and the damage may not show up until it affects care decisions.
Imaging workflows have a similar weak spot. A PACS-connected labeling tool could add slight artifacts to chest CTs or mammograms while marking them as no finding. The model then learns the wrong pattern, and each retraining cycle can deepen the mistake.
What makes these attacks hard to catch is how little poison they need. Research in healthcare AI poisoning found that as few as 250–300 poisoned images in 1 million training samples - about 0.025% of the dataset - can embed a backdoor.[7] In medical LLM research, swapping just 0.001% of training tokens with medical misinformation made models more likely to generate clinically harmful text.[10][11]
Compromised Checkpoints, Fine-Tuning Artifacts, and Backdoored Models
Pre-trained medical models and vendor-delivered checkpoints bring a different kind of risk. Many healthcare AI teams pull in external weights and fine-tune them on local clinical data. In practice, that means treating the base model like a trusted supply chain object. That trust may be misplaced.
A backdoored checkpoint can sail through standard validation. On clean test data, the model looks normal. But if it sees a rare trigger - maybe a phrase in free text like reassure family about normal results, a certain pixel watermark in imaging, or a particular mix of patient metadata fields - it can produce unsafe outputs in a systematic way.[8][9] Clinical validation tends to focus on average performance in common cases, so these triggers can slip by and stay hidden until the model is live.
Tampered intermediate artifacts can do the same kind of damage. Split checkpoint files, training scripts, or hyperparameter configs may cause a model to suppress alerts or lower risk scores under certain input combinations. Those attacks can dodge routine monitoring for months.[7] Healthcare organizations should treat outside checkpoints and fine-tuning packages the same way they treat any third-party software component in the supply chain.
Risk Indicators and Control Points for Training Integrity
Finding a compromised data pipeline means watching signals that many security teams still miss. The clearest warning signs include:
- unexplained performance drift after retraining
- inconsistent model behavior across facilities or demographic groups with no clear clinical reason
- anomalies in ETL logs, such as sudden shifts in lab value distributions or spikes in late EHR edits
- unusual access to training datasets or labeling tools by non-clinical accounts[5][6]
A few control points matter most here. Track provenance. Check integrity before retraining. Lock holdout sets. Require documented sign-off before deployment. A clean holdout set helps stop poisoned data from affecting both training and evaluation at the same time. It also helps to use centralized tracking for data lineage, retraining approvals, and audit evidence across every model version.
Once the model goes live, the attack surface moves from training integrity to prompts, outputs, and clinical workflows.
Stage 2: Deployed Model and Clinical Interface Attacks
After training integrity, the next danger point is the live clinical interface. Once a model is in use, the threat changes. It’s no longer mainly about poisoned training data. Now the problem is manipulated inputs, outputs, and tool actions. In plain terms, the attack surface becomes the way users, documents, and day-to-day clinical workflows can steer a deployed system off course.
Prompt Injection in Generative Clinical Assistants and Tool-Using Agents
Prompt injection is a major threat in deployed clinical AI. It shows up in two main ways. In a direct injection, an attacker types instructions into the chat or input field to override the model’s built-in rules. In an indirect injection, the harmful instruction is tucked inside content the model retrieves, such as a clinical note, a PDF policy document, or a referral letter.[3][15][17]
This is not a fringe issue. Prompt injection worked in 94.4% of trials across commercial medical LLMs, including high-harm cases like unsafe pregnancy drug advice and dangerous drug combinations.[12] In agentic systems, a single injected instruction can set off unsafe EHR actions or patient messages.[3][4][17]
That same interface can also leak training data through repeated probing and retrieval abuse.
Model Inversion, Membership Inference, and PHI Exposure
Query-based attacks don’t need internal access. API access alone may be enough. An attacker can probe a model to infer whether a specific patient record was part of training. That’s the core issue with membership inference and model inversion, and it can expose PHI, create HIPAA breach exposure, and increase re-identification risk.[13]
RAG systems add another weak spot. Crafted queries can pull out retrieved EHR content, including names, dates, and record fragments. That can turn data that looked de-identified back into individually identifiable health information. In other words, Safe Harbor de-identification standards can fail in practice, and breach notification duties may follow.[13][14][16]
Risk Indicators and Safeguards for Clinical AI Use
Security and compliance teams should watch for a small set of warning signs in logs and output monitoring. Some red flags are pretty blunt:
- Override phrases like
ignore previous instructionsoryou are not bound by hospital policies - Strange Unicode sequences or encoded strings in patient-submitted messages
- Tool calls triggered by routine-looking queries
- Assistant outputs that suddenly drift from clinical guidelines after a certain document is introduced[3][4][15][17]
Controls need to match the risk. Useful steps include prompt isolation, input sanitization on all retrieved content, output filtering for PHI and unsafe clinical advice, query throttling to limit repeated probing, and endpoint logging with audit trails. For high-impact actions like order placement, patient messaging, and care plan updates, human-in-the-loop review is not optional. Red-teaming should also test injection through patient-controlled fields, session notes, and retrieved documents as part of any clinical AI deployment plan.[18][19]
The next exposure layer comes from vendor models, plugins, and embedded AI modules.
Stage 3: Third-Party AI Components and Supply Chain Compromise
Once AI moves outside the hospital’s own build path, the risk changes shape. It starts to live in vendor files, connectors, and update cycles. Most healthcare groups don’t build AI systems from the ground up. They buy them, license them, or get them through EHR upgrades and imaging platform bundles. So supplier review is part of the AI attack surface. It’s not just a procurement checkbox.
Vendor-Supplied Models, Plugins, and Embedded AI Modules
At this stage, the weak spots often sit inside vendor artifacts, connectors, and update paths. When a health system rolls out a vendor model, EHR-embedded CDS, or a cloud-hosted patient chatbot, it also takes on the vendor’s security choices - and the vendor’s mistakes.
Here’s the problem in plain terms: if a vendor pulls a pre-trained model from a public model hub and skips integrity checks, that model enters clinical workflows without a proper review. If it was compromised before the hospital even bought it, the flaw comes along for the ride.
Connectors are another weak link that often gets less attention than they deserve. FHIR interfaces, HL7 bridges, and custom APIs that connect hospital systems to outside AI engines can be abused to inject adversarial inputs or malformed data. That can skew risk scores, corrupt EHR summaries, or slip attacker-written text straight into the medical record. One compromised link in the vendor stack can ripple across the full clinical workflow.
What to Look for in AI Supply Chain Risk Reviews
Standard HIPAA questionnaires and generic cyber reviews miss a lot of AI-specific risk. Procurement, security, and compliance teams need to ask sharper questions.
The biggest warning signs usually show up when a vendor can’t clearly explain its training data. If it can’t say what data trained the model, the time range of that data, or the de-identification method used, that’s a problem. Another major gap is weak AI-specific incident response language. If there’s no clear promise to notify customers when a model is compromised or tainted data is found, that should set off alarms.
Other signs deserve close review too:
- Unclear PHI retention and fine-tuning practices
- Unpatched AI-related APIs
- Undocumented model update cycles
- No visibility into fourth-party vendors, such as model hubs, cloud LLM providers, or plug-in ecosystems the vendor depends on
An AI bill of materials should be a requirement. It should cover training pipelines, serving stacks, and any third-party weights or datasets.
Governance and Continuous Oversight Across the Vendor Ecosystem
A one-time vendor review won’t keep up with AI systems that change all the time. For the risks already on the table - compromised artifacts, weak connectors, and hard-to-trace training pipelines - continuous oversight means reassessment when updates happen, drift monitoring, and clear escalation paths across security, privacy, clinical, and legal teams.
Contracts should spell out model documentation requirements, limits on PHI use for training, breach timelines, and subcontractor controls.
These three patterns can help teams structure vendor review:
| Compromise Type | Healthcare Touchpoint | Risk Indicators | Governance Controls |
|---|---|---|---|
| Compromised model artifacts (poisoned weights, backdoored checkpoints) | Radiology AI, diagnostic decision support | Vendor pulls from public model hubs; no integrity verification; unexplained performance shifts after updates | Require an AI bill of materials; mandate adversarial testing evidence; reassess after major model updates |
| Vulnerable plugins and connectors (FHIR bridges, HL7 interfaces, API integrations) | EHR-embedded CDS, scheduling optimization, patient triage tools | Unpatched APIs; undocumented connector changes; malformed data accepted without validation | Use least-privilege access for AI tools; test connectors; log all integration-layer inputs and outputs |
| Opaque vendor training pipelines (unknown data sources, unclear PHI handling) | Clinical chatbots, documentation assistants, SDoH-informed risk models | Missing data provenance; no model card; no fourth-party disclosure | Require detailed training-data lineage; include AI-specific BAA addenda; continuously monitor through a unified risk dashboard |
Conclusion: A Practical Control Model for Reducing Healthcare AI Risk
Healthcare AI attacks hit the entire lifecycle, not just one app or one model. Bad training data, prompt injection, and tampered vendor models can all shift how a system behaves without causing an obvious outage. That’s why the defense has to cover the same lifecycle from end to end.
In plain English: it’s time to move from describing threats to putting day-to-day controls in place.
Key Actions for Security, Compliance, and AI Governance Leaders
Start with a central inventory of every AI system that touches patient data. Then map the attack surface for each one, including embedded vendor tools inside the EHR or imaging stack. From there, group controls around four priorities:
| Priority Area | What to Do |
|---|---|
| PHI exposure classification | Tier use cases by sensitivity, volume, and external access; apply stricter controls to live clinical decision support |
| Training and pipeline integrity | Monitor data quality, verify model-artifact integrity, and run adversarial testing before deployment and after major updates |
| Vendor and fourth-party review | Require model origin, training-data provenance, and external-component disclosure; reassess after updates |
| Deployment and clinical use controls | Enforce input validation, output monitoring, and human review for high-consequence actions |
There’s a catch: none of these controls work if no one owns them.
Governance is what turns policy into action. An AI oversight committee with people from security, compliance, privacy, clinical safety, IT, and data science needs clear decision rights and a set reporting rhythm. Without that, even well-written controls can sit on the shelf.
And the risk here isn’t theoretical. Prompt injection worked in 94.4% of simulated clinical LLM interactions in one study [12], while data poisoning placed a backdoor into a radiology model using only 0.025% of the training set [1][2]. That’s why centralized oversight, staged testing, and lifecycle-aware controls matter so much: they help teams catch failures before those failures touch a patient.
FAQs
How would a healthcare AI attack show up in day-to-day clinical use?
In clinical settings, a healthcare AI attack often doesn't look like a loud security incident. It looks like a quiet pattern of failure.
The system may appear to run as usual while giving misleading outputs that are hard to catch in the moment.
That can show up as skewed recommendations, imaging misclassifications, or odd behavior in triage and scheduling. In some cases, the model may display deceptive behavior only when certain inputs appear, which makes the problem even harder to spot.
And that's the dangerous part: these issues can stay hidden for 6 to 12 months or longer.
What makes prompt injection so dangerous in healthcare AI?
Prompt injection is dangerous in healthcare AI because it uses runtime inputs - like metadata, clinical notes, or imaging data - to change how a model behaves without setting off standard security alerts.
That’s what makes it so risky. The input can look harmless on the surface, yet still slip past common defenses. In a healthcare setting, that can lead to unsafe clinical recommendations, exposed patient data, or system actions that no one approved through EHR or tool-calling integrations.
What should we ask vendors about AI security and PHI use?
Go beyond standard compliance checklists.
Ask:
- What data is used to train or refine the model?
- Where does that data go, including third- and fourth-party sub-processors?
- Who can change model parameters or weights after deployment?
Require a BAA for any vendor accessing PHI. If a vendor refuses, keep that tool out of PHI workflows.
Also review change control for adaptive AI, along with documentation that covers AI supply chain security.
