AI attacks can change model behavior without malware, account takeover, or network break-ins. That’s the core issue. If I rely on the old seven-step kill chain alone, I miss how AI gets hit through data poisoning, prompt injection, adversarial inputs, model theft, and vendor-linked model changes.
Here’s the short version:
- Old cyber models focus on hosts, accounts, and network traffic
- AI attacks often hit data, prompts, models, and outside services instead
- Damage can happen before deployment, during inference, or through vendor updates
- In healthcare, bad AI output can affect patient safety, not just security
- What works better is lifecycle-based risk mapping across data, model, app, and vendor layers
A simple example: a hospital system could have 0 malware alerts, 0 C2 events, and 0 server compromises - and still end up with a model that gives unsafe advice because training data was altered or a prompt changed runtime behavior.
That’s why I’d treat AI risk as a behavior and data problem, not just an IT intrusion problem.
What this means for you:
- Inventory every AI system
- Assign business and security owners
- Extend vendor reviews to cover AI data sources, models, prompts, and fourth parties
- Log prompts, outputs, model versions, and PHI access paths
- Test for prompt injection, model extraction, and poisoned data on a set schedule
[RISK] Why AI Agents Will Break Your Security Kill Chain | #NEWIT
sbb-itb-535baee
Quick Comparison
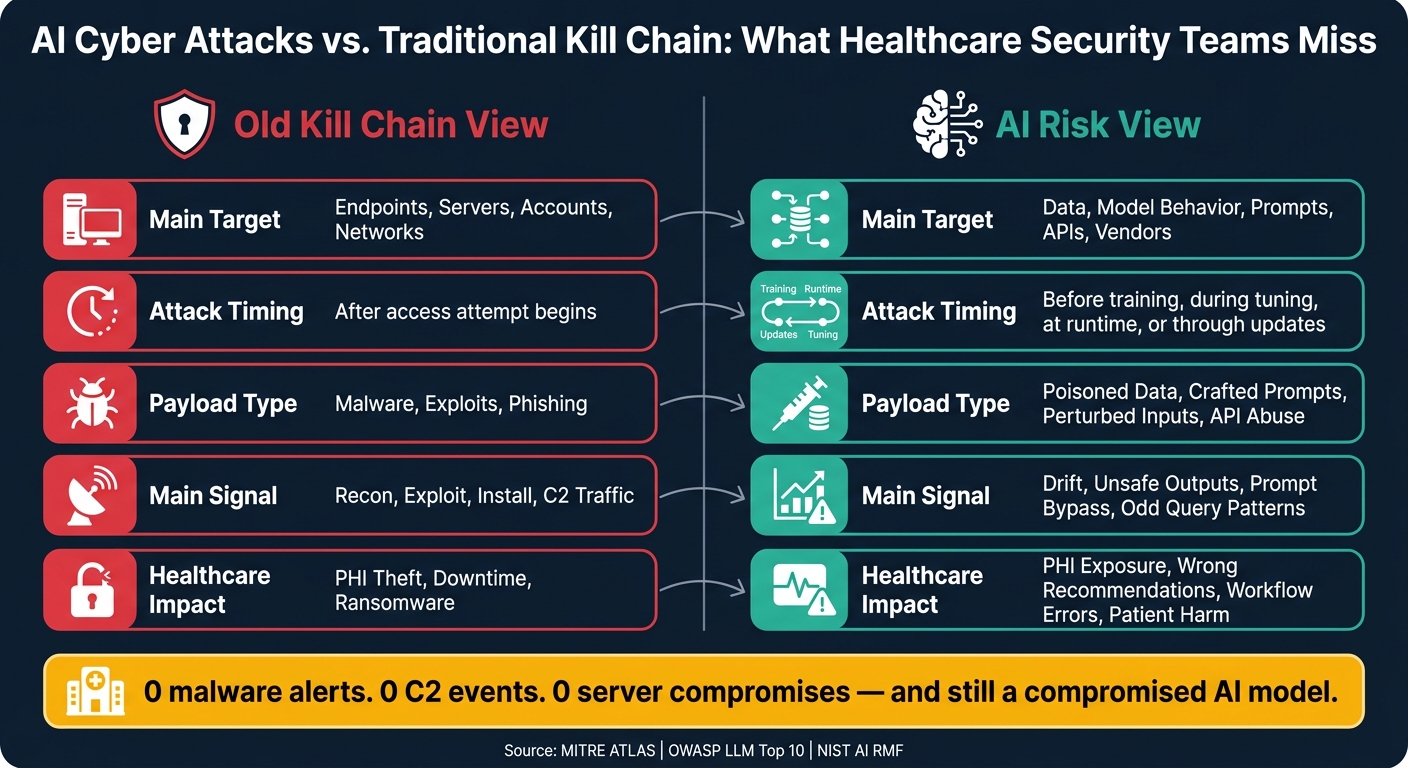
AI Cyber Attacks vs. Traditional Kill Chain: What Healthcare Security Teams Miss
| Area | Old Kill Chain View | AI Risk View |
|---|---|---|
| Main target | Endpoints, servers, accounts, networks | Data, model behavior, prompts, APIs, vendors |
| Attack timing | After access attempt begins | Before training, during tuning, at runtime, or through updates |
| Payload type | Malware, exploits, phishing | Poisoned data, crafted prompts, perturbed inputs, API abuse |
| Main signal | Recon, exploit, install, C2 traffic | Drift, unsafe outputs, prompt bypass, odd query patterns |
| Healthcare impact | PHI theft, downtime, ransomware | PHI exposure, wrong recommendations, workflow errors, patient harm |
If I’m reviewing AI in healthcare, I should stop thinking in a straight line and start tracking the full AI lifecycle instead.
AI Attack Methods the Classic Model Misses or Undercounts
The biggest gaps show up in three places: upstream data corruption, runtime input manipulation, and dependency exposure.
Data Poisoning and Third-Party Data Supply Chain Risk
Data poisoning is a provenance problem, not a perimeter problem. An attacker doesn't need to break into a hospital network to do damage. They can tamper with training, tuning, or retrieval data before the model ever goes live.
That can happen in a few different ways. An insider might quietly flip labels in an internal radiology dataset. A licensed data provider might have its own environment compromised without anyone noticing. Or a public medical repository could feed misleading dosage details into a retrieval-augmented generation (RAG) pipeline used by a clinical copilot.
MITRE ATLAS documents this as "Poison Training Data" (AML.T0020), where attackers inject malicious examples into training data to plant backdoors that trigger only under certain conditions while looking normal on most inputs. [2][3][4] That's what makes this attack hard to spot. The bad data can look clean, valid, and routine, so classic endpoint and network controls often miss it.
The timing matters too. This attack lands before deployment, outside the old exploit-and-install sequence.
Prompt Injection, Adversarial Inputs, and Runtime Manipulation
Prompt injection is a runtime input attack. In plain terms, malicious text can override an LLM's instructions without any privilege escalation.
OWASP's 2025 LLM guidance lists prompt injection as a top application-layer risk for large language models because user-controlled input can override the model's intended logic without any privilege escalation. [6][7][9] That's a big deal in healthcare, where a model may be reading clinical documents, patient messages, or uploaded files in the middle of care.
A simple example shows the problem. An attacker could hide instructions inside a PDF clinical guideline that tells a RAG-enabled copilot to ignore safety rules and always recommend a certain drug for chest pain. The copilot follows the hidden instruction instead of the clinical one. No malware. No broken login. Just bad text moving through an allowed channel.
In healthcare, that means harmful guidance can enter during care, not only during system compromise.
Adversarial inputs create a related problem. Tiny, near-imperceptible changes to imaging inputs can flip a diagnostic model's output even when the image still looks normal to a clinician. Those changes can come through compromised PACS data, a patient upload portal, or sensor telemetry.
NIST's Adversarial Machine Learning taxonomy treats evasion as its own attack class and notes that attacks can happen at training, inference, and supply-chain stages, not only during exploit or installation. [1][5] Since no binary runs and no network beacon fires, endpoint and network tools built around the classic kill chain may register nothing more than normal user activity.
Once attackers can shape outputs, the next issue is whether they can steal the model or reach it through a vendor dependency.
Model Theft and External AI Dependency Exposure
Model theft can look like ordinary API use. Repeated queries may let an attacker reconstruct a deployed model, and weakly protected storage may expose model weights outright. If the model was fine-tuned on sensitive patient data, extraction can also support membership inference attacks that reveal whether data from specific people was part of the training set.
Healthcare teams also inherit vendor and subvendor risk. One compromised SaaS AI provider - whether it supports clinical decision support, radiology AI, or patient engagement tools - can poison updates or shift behavior across many customers at once.
These attack paths differ in timing, input channel, and control point.
| Attack Type | Primary Attack Vector | Where It Occurs | Why the Kill Chain Undercounts It |
|---|---|---|---|
| Data Poisoning | Corrupted training, tuning, or RAG data from insiders, compromised vendors, or poisoned public sources | Upstream data pipelines; data vendor environments; public medical repositories | Happens before old delivery/exploitation stages; the issue is data provenance and trust, not malware or a host intrusion |
| Prompt Injection | Malicious or hidden instructions in user inputs, documents, or web content | Inference-time copilots, chatbots, and triage tools | Uses allowed input channels; the payload is natural language, so there is no OS-level exploit or installation |
| Adversarial Inputs | Subtly perturbed images, signals, or text crafted to induce misclassification | Medical imaging systems, PACS archives, sensor telemetry, telehealth portals | No software flaw has to be exploited; the manipulation happens at inference and may look like normal input |
| Model Theft | API abuse, model extraction, insecure weight storage, overexposed integrations | Deployed model APIs, cloud storage, external portals | Can resemble normal API use and may be missed by intrusion-focused controls |
| Third-Party Model Risk | Vendor compromise, shared tenancy, uncoordinated model updates, fourth-party dependencies | Vendor-hosted AI platforms; SaaS clinical AI services | The classic model is organization-centric and network-centric; it does not account for upstream model compromise or cascading multi-tenant effects |
Why Healthcare AI Raises the Stakes
When AI fails in healthcare, the fallout can hit patients fast. A bad output can delay a diagnosis, steer a medication choice in the wrong direction, or miss an urgent event. So this isn't just an IT problem. It's a patient-safety problem.
Patient Safety, PHI, and Clinical Workflow Disruption
Research on medical LLMs shows that adversarial prompts and fine-tuning attacks can change AI outputs across disease prevention, diagnosis, and treatment tasks. In plain terms, the model can be pushed to give advice that discourages vaccination, suggests harmful drug combinations, or recommends imaging that isn't needed. [13] In radiology, the risk gets even sharper. A poisoned pneumonia-detection model tied into a hospital PACS could return false negatives for certain patient groups. [12]
That risk doesn't stay on the screen. It moves through care.
Take a documentation assistant. If it leaves an allergy out of a clinical note, the next clinician may trust that note and act on bad information. That's how a patient-safety event starts. Because AI now sits inside clinical workflows, one flawed output can ripple into orders, care plans, and discharge decisions before anyone spots the problem. And these failures happen during normal use, which means they often sit outside the classic kill chain's focus on networks and endpoints.
Privacy problems follow the same path. AI tools are often linked to the EHR and handle PHI through external APIs and cloud models. If an LLM assistant logs PHI in telemetry storage that doesn't meet the rules, that can become a reportable disclosure even when the EHR itself was never touched. The Joint Commission has said plainly that healthcare organizations must make sure AI uses of patient information follow HIPAA Privacy, Security, and Breach Notification Rules. [11] HIPAA's Security Rule doesn't lock teams into one type of tool or setup, so organizations still have to apply reasonable safeguards to AI workflows. And the same issue can spread through the vendors and subvendors behind healthcare AI.
Enterprise, Third-Party, and Subvendor Exposure in Healthcare
A typical HDO doesn't rely on one AI system. It often uses several vendor tools, and each one comes with its own model, data flows, and cloud setup. That means one compromised vendor can spread poisoned data or bad model behavior across many hospitals at the same time. The attack surface no longer stops at the hospital's edge. It stretches across every model, connector, and data source in the chain.
This is where static reviews start to fall apart.
These systems keep changing, so the review process has to keep up. A one-time vendor check won't catch a moving target. Models get retrained. Prompts and guardrails change. New tools and connectors get added. Outside data sources shift over time. A vendor that looked safe when the contract was signed may later roll out a new model version that handles PHI in a different way, add a web-search tool that opens up more prompt injection risk, or change its RAG knowledge base in ways the HDO never sees. Static third-party reviews miss those shifts between assessments. Managing third-party AI risk in healthcare requires tracking change, not just vendors.
A Better Approach: AI-Specific Risk Mapping and Governance
AI risk doesn’t stay still. It shifts as data changes, models are updated, apps are tuned, and vendors add new dependencies. That’s why governance can’t rely on one-time reviews. In healthcare, that kind of static check misses how AI systems evolve in day-to-day use. A better path is a layer-by-layer risk map that follows the full chain: data, models, applications, and vendors.
Map AI Risk Across Data, Model, Application, and Vendor Layers
Instead of following one attack path, AI risk mapping should cover four connected layers:
- Data layer: Track data provenance, access, and drift in training and inference inputs.
- Model layer: Track model version, retraining, fine-tuning, and known limits through a model bill of materials (BoM).
- Application layer: Control prompts, review high-risk outputs, and log sessions for response and audit.
- Vendor layer: Inventory external models, APIs, data providers, and fourth-party dependencies.
The FDA treats AI management as an iterative lifecycle, from design through maintenance.[16] Mapping risk across these four layers puts that idea into day-to-day practice.
That map should then feed both vendor reviews and internal assessments.
Updated Assessment Questions for AI-Enabled Environments
Standard security questionnaires weren’t built for AI-heavy settings. They still ask the right baseline questions about encryption, access controls, and incident response. But they often skip the issues that can make or break an AI system. The gap is pretty plain once you line the old questions up against AI-specific ones.
| Assessment Area | Standard Question | AI-Specific Question |
|---|---|---|
| Data & Training | How is data encrypted at rest and in transit? | List all training and fine-tuning data sources and their governance controls for PHI. |
| Model Lifecycle | What is your patch management process? | Provide a model BoM for each AI model in service. |
| Prompts & Outputs | How do you prevent unauthorized data access? | How do you prevent, detect, and respond to prompt injection and adversarial inputs? |
| Logging & Retention | What events do you log and for how long? | What prompts, inputs, and outputs are logged, retained, and audited? |
| Vendor & Fourth-Party | Do you use subcontractors? | List all third- and fourth-party AI services and data providers, and how you monitor them. |
These questions can be folded into vendor assessments and internal reviews. They don’t replace standard security checks. They extend them so they fit AI-enabled environments.
Governance Actions Healthcare Leaders Can Put Into Practice
Start with an AI inventory. Every system should be listed with the data it touches, the person who owns it, and the vendors behind it. Without that, governance is working blind. Build the inventory through department surveys and by reviewing vendor lists, integrations, and contracts. Shadow AI and pilot projects need to be in scope too, not just approved enterprise tools.
Next, assign two owners to each AI system: a business owner and a security owner. The business owner - for example, the CMIO for clinical decision support - owns the use case and clinical safety. The security owner is accountable for controls and compliance. ECRI lists insufficient AI governance as one of its top 10 patient safety concerns for 2025.[17] So this isn’t only an IT issue. It reaches patient safety as well.
Assessment findings should move into a formal oversight structure. The NIST AI RMF frames this work around Govern, Map, Measure, and Manage.[14][15] Under Govern, that means setting policies, roles, and escalation paths. Under Measure, it means watching for model drift, adversarial traffic, and prompt injection attempts over time. Platforms like Censinet RiskOps and Censinet AI can help by keeping the AI inventory up to date, sending AI-specific vendor questionnaires, routing findings to the right stakeholders - security, privacy, and clinical leaders - and giving teams centralized dashboards to view AI risk posture across the enterprise. Those findings should then shape the control priorities below.
Controls for AI-Enabled Environments and Conclusion
Control Priorities for Healthcare AI Deployments
Governance has to lead the way. Start with your data, model, application, and vendor map, then pick controls by layer. Each layer stops a different kind of AI attack.
Input validation comes first. Check all inputs - lab values, notes, PDFs, and DICOM images - before they ever touch the model.[9][18][20] Then add prompt and output filtering to catch what slips through. A separate policy engine can block PHI, unsafe advice, and instruction overrides before users see the output.[18]
In retrieval-augmented generation (RAG) systems used for clinical decision support, retrieval hardening matters just as much. Least-privilege access to EHR and imaging systems, query whitelisting, and role-based document limits can stop a prompt injection from spreading too far.[9] For access control, store API keys in hardware-backed vaults, use RBAC for model endpoints, and require MFA for model changes.[20][21]
You also need a clear record of what happened. Log prompts, tool calls, outputs, model versions, and PHI access paths in immutable logs.[8][18][19][20] Watch those logs for signs that something is off, like unusual export activity, repeated safety-bypass attempts, or spikes in PHI queries. On top of that, run recurring AI red-team tests for prompt injection, adversarial imaging inputs, and model extraction with clinical, security, and compliance staff involved.[8][19][20]
Control Matrix: Major AI Threats and the Most Relevant Mitigations
Match each major threat to the control most likely to stop it.
| AI Threat | Primary Controls | Healthcare-Specific Notes |
|---|---|---|
| Data poisoning | Data provenance tracking, anomaly detection on training pipelines, golden dataset validation, change control for retraining | Treat poisoning as both a security and patient safety issue; involve clinical quality teams |
| Prompt injection | Input validation, prompt filtering, retrieval hardening, least-privilege tool access | Apply to all input channels: patient portals, clinician interfaces, and third-party content sources |
| Adversarial inputs | DICOM/signal validation, adversarial robustness testing, red-teaming for imaging models | Diagnostic models are high-stakes targets; test with realistic clinical scenarios |
| Model theft | RBAC, MFA, secrets management, API rate limiting, encrypt model artifacts, export monitoring | Monitor for systematic querying patterns that resemble model extraction |
| Third-party AI risk | AI-focused vendor due diligence, fourth-party inventory, contract SLAs for incident notification, sub-processor attestations | Require SOC 2, HITRUST, or ISO 27001 for critical sub-processors and contract for rapid AI incident notification[10] |
Conclusion: Move from Linear Thinking to Lifecycle-Based AI Risk Management
These controls do not help much if they sit on paper and never get reviewed. AI attacks don’t follow the old kill chain in a neat, straight line. Data can be poisoned before training starts. Prompts can steer behavior during runtime. Models can leak through APIs. Vendors can bring in risk through dependencies that never show up in a standard asset inventory.
In healthcare, the stakes are higher. PHI, clinical workflows, and patient safety outcomes are all part of the picture. A misconfigured AI system or a poisoned dataset is not just an IT problem. It is a patient safety problem. HIPAA compliance by itself does not close that gap.[8]
Update AI risk reviews now. Inventory every AI system, assign ownership, extend vendor assessments to cover AI-specific risks, and monitor them over time. Linear thinking built for conventional IT won’t protect AI-enabled environments. Lifecycle-based risk management will.
FAQs
What is the biggest blind spot in the traditional kill chain for AI?
The biggest blind spot is simple: old-school kill chain models were built for fixed software and infrastructure attacks. AI systems don't work that way. They can be pushed off course through their own internal logic and decision-making.
That changes the game.
Traditional security tools often miss AI-specific threats like data poisoning and adversarial inputs because those attacks can look normal on the surface. Nothing obvious breaks. No alarm goes off. But under the hood, a compromised model can still shape clinical decisions without being detected.
How can a healthcare AI system fail without any malware or breach?
A healthcare AI system can break down even when there’s no malware and no security breach. Sometimes the problem comes from weak spots in the data, the model’s logic, or the setting where the system runs.
That can show up in a few ways:
- Data poisoning, where bad or misleading data gets into the training set
- Adversarial inputs, where small changes in input data push the model toward the wrong output
- Model drift as patient demographics or clinical protocols change over time
- Accidental PHI exposure when staff paste sensitive data into public, unapproved AI tools
In plain English, the system may look fine on the surface, but the results can still go off track if the inputs shift, the model falls out of step with current care patterns, or people use tools they shouldn’t.
What should healthcare teams monitor first in AI systems?
Healthcare teams should start with AI risk assessments that cover the entire model lifecycle, from data collection and training to deployment and continuous monitoring. A one-time review isn't enough. AI systems change over time, and so do the risks around them.
That means looking at a few core areas in a connected way:
- Centralized AI governance so decisions, ownership, and oversight don't get scattered across teams
- The full AI supply chain, including data sources, model components, tools, and outside partners
- AI-specific vendor due diligence that goes beyond standard IT or security checks
- Continuous monitoring for drift, performance issues, and anomalous inputs after deployment
In plain terms, healthcare organizations need a clear process for checking how an AI system is built, where its parts come from, how outside vendors handle risk, and what happens once the model is live. Without that kind of end-to-end review, problems can slip in quietly and grow over time.
