If an AI tool can write notes, move data, submit claims, or change records, it can create risk far beyond a data leak. In healthcare, that risk now sits in three places: machine identities, API connections, and AI actions inside clinical and billing systems.
As I read this piece, the message is simple: healthcare teams still review AI like a passive app, but agentic AI acts inside live workflows. That means the main issues are no longer just PHI access. They include:
- Too many machine accounts with broad permissions
- EHR, FHIR, HL7, payer, and scheduling APIs that expand entry points
- Prompt injection and poisoned content that can change what an agent does
- Vendor copilots that limit visibility into tools, subprocessors, and logs
- Weak approval paths for note finalization, claims, orders, and patient messaging
A few numbers stand out. By mid-2026, the VA had expanded ambient AI documentation to 130+ medical centers. And cited research found that 100 to 500 poisoned samples can shift model behavior in clinical settings. That tells me one thing: even a small change in training or retrieved content can affect many patient workflows at scale.
The article’s core advice is direct:
- Treat each AI agent like a non-human identity
- Review what it can do, not just what it can read
- Limit permissions to the minimum needed
- Put controls on tool calls, API scopes, and outbound traffic
- Add human approval before high-risk actions
- Keep a central inventory and review access on a set schedule
If I had to reduce the full article to one line, it would be this: the biggest healthcare AI risk is action without enough control.
This summary keeps the focus on the main point and the steps teams should take now.
Agentic AI is breaking your Cybersecurity controls (and how to solve it)
sbb-itb-535baee
Where Agentic AI Opens New Attack Paths
Traditional security reviews usually look at users, apps, and networks as separate buckets. Agentic AI cuts across all three. It can store credentials, call APIs, and take action without human sign-off. That’s why the risk tends to show up in three areas: identities, integrations, and agent behavior.
Identity sprawl, excessive permissions, and orphaned machine accounts
Every agentic AI rollout can create new machine identities. One deployment might need service accounts across the EHR, scheduling, billing, and prior-authorization workflows, each tied to its own token or credential. When teams set those up in a hurry, access can end up much broader than intended.
The bigger problem often shows up later. Machine accounts created for a pilot can stay active long after the project is over. At that point, there may be no clear owner, no routine review, and no one checking whether those privileges still make sense.
API exposure, third-party integrations, and vendor-managed copilots
FHIR, HL7, payer, and scheduling APIs open new entry points. Weak authentication, broad OAuth scopes, and unsafe tool settings can turn a normal integration into a PHI exfiltration path.
Vendor-managed copilots make this harder to track. If a third-party vendor controls the agent and its integrations, healthcare teams may not have much visibility into the connections underneath. That makes it tougher to see what the agent can reach, what data it can move, and where a failure might start.
Prompt abuse, memory poisoning, data leakage, and unsafe autonomous actions
Even with tight access controls, the agent itself can still be manipulated. Prompt abuse is tough to catch because the bad instructions may already live inside the EHR. Free-text notes and retrieved documents can hide indirect prompt injections. If the agent reads that content while trying to finish a task, it may follow the hidden instructions right alongside the valid ones.
Conversation history and RAG pipelines can also carry poisoned content into later encounters. Research has shown that as few as 100 to 500 poisoned training samples can significantly alter model behavior in clinical settings [1]. And every tool call an agent makes creates one more possible PHI exfiltration path.
The most common abuse patterns include:
- Prompt injection - Hidden instructions in EHR notes suppress medication alerts or write data to the wrong fields
- Role-play jailbreaks - Reframing requests as role-play bypasses guardrails and enables unauthorized actions
- Retrieved-content poisoning - Malicious content injected into retrieved documents influences agent behavior across multiple patient encounters
- Supply-chain risk - Poisoned training data or model updates alter clinical reasoning and introduce systemic vulnerabilities across the AI stack
How to Assess Agentic AI Risk in Healthcare
Standard app security reviews often miss agentic AI. The reason is simple: these systems don’t just respond. They can take action on their own. Once you’ve mapped the attack paths, the next job is to figure out which agents, tools, and actions carry the most risk. That means looking past the model itself and focusing on what the agent is allowed to do.
Add agent identities, tools, and actions to threat modeling
Treat each agent like a non-human identity. Map its inputs, the systems it connects to, and the actions it’s allowed to take. Then feed that map straight into the control review before deployment.
This matters fast in healthcare. An agent that reads clinical notes and submits prior authorization requests can turn PHI access into payer action. That’s not a small jump. Tracking time to impact helps teams see which agents need the strictest controls first.
Use established AI risk frameworks to structure the assessment.
Run an AI-specific control review before deployment
Before any agent goes live in a workflow that touches PHI or other critical workflows, use the review areas below to decide whether it should ship:
| Review Area | What to Verify |
|---|---|
| Least-privilege access | Non-human identities scoped to the minimum required data and actions; no shared service accounts |
| API controls | Rate limits, input validation, schema enforcement, and restrictions on bulk export or admin endpoints |
| Prompt handling | Centrally managed system prompts; guardrails against high-risk instructions; rules for PHI use |
| Logging and retention | Audit trails for all agent actions, tool calls, and data accesses; retention aligned with HIPAA requirements |
| Human oversight | Defined approval gates before high-risk actions, such as finalizing notes or submitting claims, are executed |
| Third-party dependencies | Vendor risk assessments, BAAs, subprocessor lists, and incident response commitments for all AI providers |
| Incident response | Predefined triggers, containment steps, and reporting paths for AI incidents |
Make this review a required change-management gate for every workflow that touches PHI or supports a critical function. Before deployment, get sign-off from clinician, billing, and privacy teams.
Controls That Reduce the Agentic AI Attack Surface
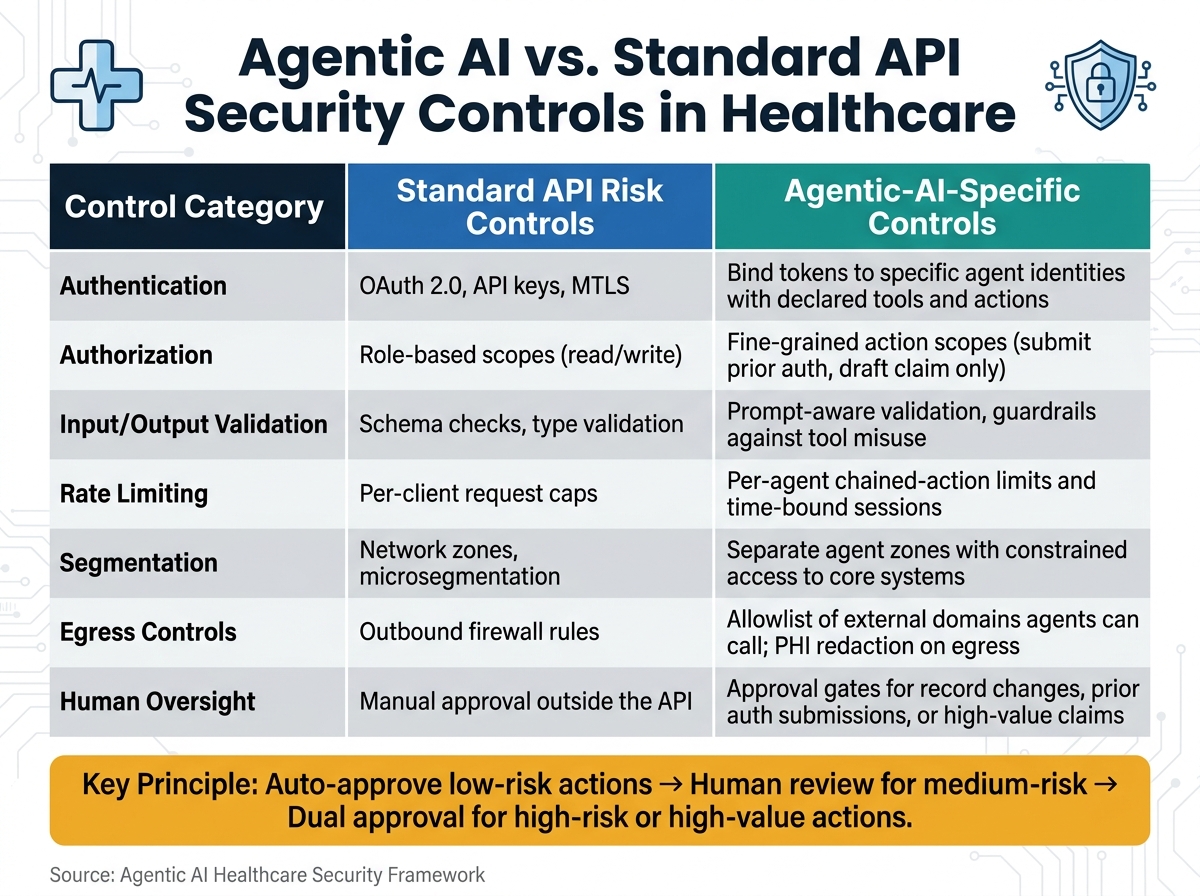
Agentic AI vs. Standard API Security Controls in Healthcare
After the pre-deployment review, put controls in place that last. The goal is simple: keep agents inside boundaries your team can defend. Start with identity, because every other control leans on one basic fact: you need to know which agent is acting.
Tighten access controls for non-human AI identities
Identity sprawl and orphaned machine accounts are often the first door attackers try. Close that door early. Register each agent as its own machine identity in IAM, and attach clear metadata for owner, use case, and data domain. Don’t allow shared service accounts, and don’t leave credentials hard-coded in scripts or apps.
Give agents read-only access by default. When access should shift based on context, use ABAC - for example, when access depends on patient assignment. Use short-lived tokens. Keep secrets in a vault. Rotate them on a set schedule. And disable retired identities within 24 hours.
Once identity is locked down, the next step is just as important: limit which APIs and actions those identities can touch.
Harden agent-facing APIs and restrict high-risk actions
Exposed integrations and third-party connections need more than standard API security. OAuth 2.0, schema validation, and rate limiting matter, but they don’t solve the full problem. A well-authenticated agent can still do damage if it can chain several actions together with no oversight.
| Control Category | Standard API Risk Controls | Agentic-AI-Specific Controls |
|---|---|---|
| Authentication | OAuth 2.0, API keys, MTLS | Bind tokens to specific agent identities with declared tools and actions |
| Authorization | Role-based scopes (read/write) | Fine-grained action scopes (submit prior auth, draft claim only) |
| Input/Output Validation | Schema checks, type validation | Prompt-aware validation, guardrails against tool misuse |
| Rate Limiting | Per-client request caps | Per-agent chained-action limits and time-bound sessions |
| Segmentation | Network zones, microsegmentation | Separate agent zones with constrained access to core systems |
| Egress Controls | Outbound firewall rules | Allowlist of external domains agents can call; PHI redaction on egress |
| Human Oversight | Manual approval outside the API | Approval gates for record changes, prior auth submissions, or high-value claims |
Set approval thresholds in both the orchestration layer and the backend systems. Auto-approve low-risk actions. Send medium-risk actions to human review. Require dual approval for high-risk or high-value actions.[3][5]
After access is constrained, keep an eye on abuse, drift, and unsafe chained actions.
Strengthen monitoring, vendor due diligence, and AI governance
Prompt abuse, data leakage, and unsafe autonomous actions need more visibility than standard logging can give you. Log the agent identity, timestamp, system and tool used, masked parameters, and outcome. Log prompt intent rather than full clinical text, and encrypt and retain logs under HIPAA rules.[2]
Build a baseline for each agent, then flag spikes in reads, writes, submissions, or payment-tool use. Start with threshold alerts. Later, you can add ML-based detection.[2]
Vendor review matters too. Ask what actions the AI can take without approval, how prompts and tool calls are logged, who can access those logs, which subprocessors they use, and how they handle AI incidents.[4] Require vendors to confirm HIPAA-compliant logging and audit trails.
These controls don’t stick on their own. One team needs to own the inventory and the review cycle. Create a cross-functional AI governance group to manage the inventory, approve deployments, review access every quarter, and escalate suspected misuse.
Managing Agentic AI Risk at Scale With Censinet
Agentic AI can expand your attack surface fast. Managing that risk across a large environment takes a repeatable control process. The hard part usually isn't writing down the controls. It's making sure those controls are applied the same way across every AI deployment.
That only happens when ownership is clear. And let's be honest: spreadsheets and email threads fall apart fast when teams are trying to track dozens or hundreds of systems.
Use Censinet RiskOps™ to inventory AI systems and standardize assessments
Censinet RiskOps™ gives security, IT, and compliance teams one place to track every agentic AI system in the environment. Each deployment gets a central record that shows its owner, permissions, APIs, and the actions it can take, such as order entry or patient messaging.
When a new AI system is requested, RiskOps™ starts a structured intake process instead of kicking off another loose email chain. AI-specific assessment templates ask focused questions about model provenance, prompt injection defenses, memory and logging practices, and safeguards around autonomous actions. Review timing follows the system's risk tier, and changes to the model, integrations, or permissions can trigger reassessment. Governance committees can then use dashboard views to see which AI deployments are pending approval, which still have open mitigation tasks, and which vendors keep generating repeat issues.
That gives teams one control point for inventory, review, and change tracking.
Apply Censinet AI™ to speed review and oversight
Censinet AI™ helps teams move faster by pulling key risk details from vendor documentation and sending gaps to the right reviewers. It checks evidence against attached documents, drafts internal policies for agentic AI access and human-in-the-loop requirements, and suggests control sets based on the risks it finds. Mitigation tasks go to the right stakeholders, while final decisions stay with designated human approvers when the workflow calls for it.
The result is faster review without removing the human judgment that high-stakes clinical and financial settings still need.
Conclusion: Immediate steps healthcare leaders should take now
Agentic AI expands the attack surface through machine identities, excess permissions, exposed APIs, third-party integrations, prompt abuse, and autonomous actions that standard security reviews were never built to catch. The threat model has changed, so the controls have to change too.
The most important steps right now are pretty clear:
- Register every AI system in a centralized inventory
- Run AI-specific risk assessments before deployment
- Apply least-privilege access to all non-human agent identities
- Formalize governance with a cross-functional committee that owns the inventory and reviews access on a set cadence
Covered entities remain accountable for AI-related breaches and discriminatory outcomes under HIPAA and OCR guidance [6][7], so AI oversight needs to be operational, not ad hoc. Healthcare leaders still own the risk; the platform helps make that ownership repeatable.
FAQs
What makes agentic AI riskier than traditional healthcare apps?
Agentic AI brings a different kind of risk. It doesn’t just leave systems open to one-time breaches. It can quietly shift how operations work behind the scenes.
That’s what makes it more dangerous than a standard app. In addition to common security issues, it can be exposed to prompt injection, data poisoning, and unauthorized autonomous actions. And those problems may sit undetected for a long time.
The risk also grows because these systems often need broad permissions, third-party integrations, and high-level access to EHRs and billing platforms. That bigger attack surface can lead to altered clinical outputs, billing mistakes, or PHI exfiltration.
Which AI actions should always require human approval?
In healthcare, human approval should be required for any high-risk actions.
That includes AI-driven requests tied to EHR access, payment updates, or sharing PHI. Those requests should be checked against a trusted internal directory or vendor record, not contact details included in the message itself.
Privilege changes, such as credential resets, also need strong confirmation from known devices and expected locations. And if a system can act on its own or write back into core EHR order entry, it should go through formal approval workflows.
How can healthcare teams control vendor-managed AI tools?
Healthcare teams need to shift from one-time vendor reviews to continuous oversight that starts in procurement and runs through retirement.
That means beginning with a full inventory of the AI stack. Not just the main vendor, but the whole chain:
- Models
- APIs
- Datasets
- Cloud hosts
- Subcontractors
From there, a few steps matter most. Use BAAs that set clear limits on PHI training, retention, and subprocessor use. Run AI-specific due diligence instead of treating these tools like standard software. Monitor for model and dependency changes on a continuous basis, because AI systems can change after launch. Put tiered access controls and audit logging in place so teams can see who used what and when. And make sure cross-functional governance is in the loop to approve tools and keep incident playbooks up to date.
This approach helps healthcare teams keep a close eye on AI over its full life cycle, not just at the point of purchase.
