AI vendor risk in healthcare is not just software risk. If a model can change after launch, pass PHI through prompts or logs, or depend on outside providers you never approved, your current vendor review process can miss the biggest problems.
Here’s the short version:
- AI tools rely on layered vendors like model providers, cloud hosts, data-labeling firms, and EHR add-ons.
- Those hidden links can affect care, privacy, and compliance even if your contract covers only one vendor.
- Old vendor checks miss AI-specific risks like drift, prompt injection, cross-customer data reuse, and PHI leakage in logs.
- Healthcare teams need a different review process built around:
- data lineage
- PHI use and retention
- model updates
- human review
- continuous monitoring
One stat stands out: healthcare still has the highest data breach costs of any industry. Add AI to that mix, and the risk is no longer limited to IT. It can shape diagnosis, triage, billing, discharge, and patient messaging.
If I were boiling this article down to the core message, it would be this:
You should treat AI vendor oversight as a patient-safety, privacy, and compliance job from day one.
A simple way to think about it:
| Area | What to check | Main risk |
|---|---|---|
| Vendor chain | Model providers, cloud services, labeling firms, APIs | Hidden third and fourth parties |
| Data use | PHI in prompts, logs, training, and retrieval flows | PHI exposure or reuse |
| Model change | Retraining, drift, update notices, rollback plans | Output errors after launch |
| Use in care | Human review, testing, escalation paths | Unsafe clinical or coverage decisions |
So instead of asking only, “Is this vendor secure?” I’d ask:
- Who else is in the stack?
- Where does PHI go?
- Can customer data train shared models?
- What happens when the model changes?
- Who reviews outputs before they affect care?
That shift is the whole point of the article.
The problem: where AI supply chain risk appears and why it differs
Hidden dependencies: foundation models, data brokers, labeling vendors, and embedded AI features
Most healthcare AI tools run on stacked services: foundation models, ASR engines, retrieval sources, labeling vendors, and cloud APIs. Many of these never show up in the main contract. So the risk isn't just hidden. It's spread across vendors, models, and data flows.
Take ambient clinical documentation. One tool might depend on a third-party ASR engine, a foundation model hosted on a major cloud platform, and an external medical knowledge base for retrieval-augmented generation (RAG). Each layer can shape diagnosis, documentation, billing, or patient communication. And each layer may touch PHI. But the healthcare organization usually signs with only the top-level vendor.
Imaging AI and clinical decision support tools have their own chain of dependencies too. That can include annotation vendors that labeled training images, outside algorithm marketplaces, and EHR data feeds that may send PHI to models running in shared cloud environments.
Healthcare AI needs an ingredient-level inventory: who built the model, what data trained it, and which APIs and cloud services it uses.
Those hidden layers turn into clinical risk when a model changes, gets manipulated, or exposes PHI.
AI-specific failure modes: model drift, prompt injection, unreliable outputs, and PHI exposure
AI failure modes come from the way these systems work. That means they need constant management, not a one-time fix.
Model drift is a clear case. A radiology triage tool may perform well when it goes live, then slowly lose sensitivity for some pathologies over time. No one may have changed the code at all. Instead, the patient mix changed, imaging protocols shifted, or an upstream model update altered the data distribution. Research on clinical AI deployment shows that harmful data shifts and model drift are common, and they need dedicated monitoring pipelines before they affect patient care.[5]
Prompt injection is a different threat. In a patient chatbot, a user - or even content pulled in from an outside source - can include instructions that push the model away from its safety rules. Studies on LLM prompt injection in medical settings show that models are open to both direct and indirect injections, and that these attacks can slip past simple content filters, leading to unsafe outputs and policy violations.[6] In clinical decision support, injected content inside an imported clinical note could bend a recommendation chain in ways that are hard to spot later.
PHI exposure through logging is more subtle, but no less serious. AI systems often store full conversation transcripts, audio, or intermediate model states for debugging. A study of generative AI attacks against healthcare applications found that 90% of successful attacks led to leakage of sensitive data, including system prompts that contained patient information.[7]
Researchers also found cross-user leaks, where sensitive data entered in one patient session appeared in another patient's session.[7] That's a very different kind of failure. Standard web application controls were not built to catch it.
Why standard assessments miss these risks
These risks are operational, not abstract. That's why periodic questionnaires and point-in-time audits often miss them.
A SOC 2 report can show that a vendor encrypts data at rest and manages access controls. What it usually won't show is whether customer PHI was used to fine-tune a shared model, which fourth-party annotation firm labeled the training data, or how the vendor watches for drift in production.[3][4]
The gap is built into the review process itself. Standard assessments don't require vendors to disclose training data provenance, explain shared model architecture, or document what happens to PHI moving through a RAG pipeline. They don't ask who the offshore annotation team was. They don't ask whether the foundation model provider can use ingested data for future training.
The biggest blind spots show up in a few places:
- Training data provenance: Vendors may rely on de-identified PHI, licensed datasets, or synthetic data with unclear consent models. That can create regulatory exposure if PHI was used without proper authorization.
- Customer data reuse for training: Contracts may allow vendors to use customer inputs to improve shared models. In plain English, PHI from one institution could shape outputs seen by others.
- Model drift: Performance can slip without any code change, letting diagnostic errors or flawed recommendations build up without notice.
- Prompt injection: Outside content or user inputs can manipulate model behavior, leading to unsafe clinical recommendations or data exfiltration.
A standard review can approve the vendor and still miss the model, data, and logging risks that matter most in healthcare.[3][4]
sbb-itb-535baee
Navigating AI Vendor Risks: Essential Considerations for Healthcare Organizations
The solution: a practical AI supply chain risk framework for healthcare
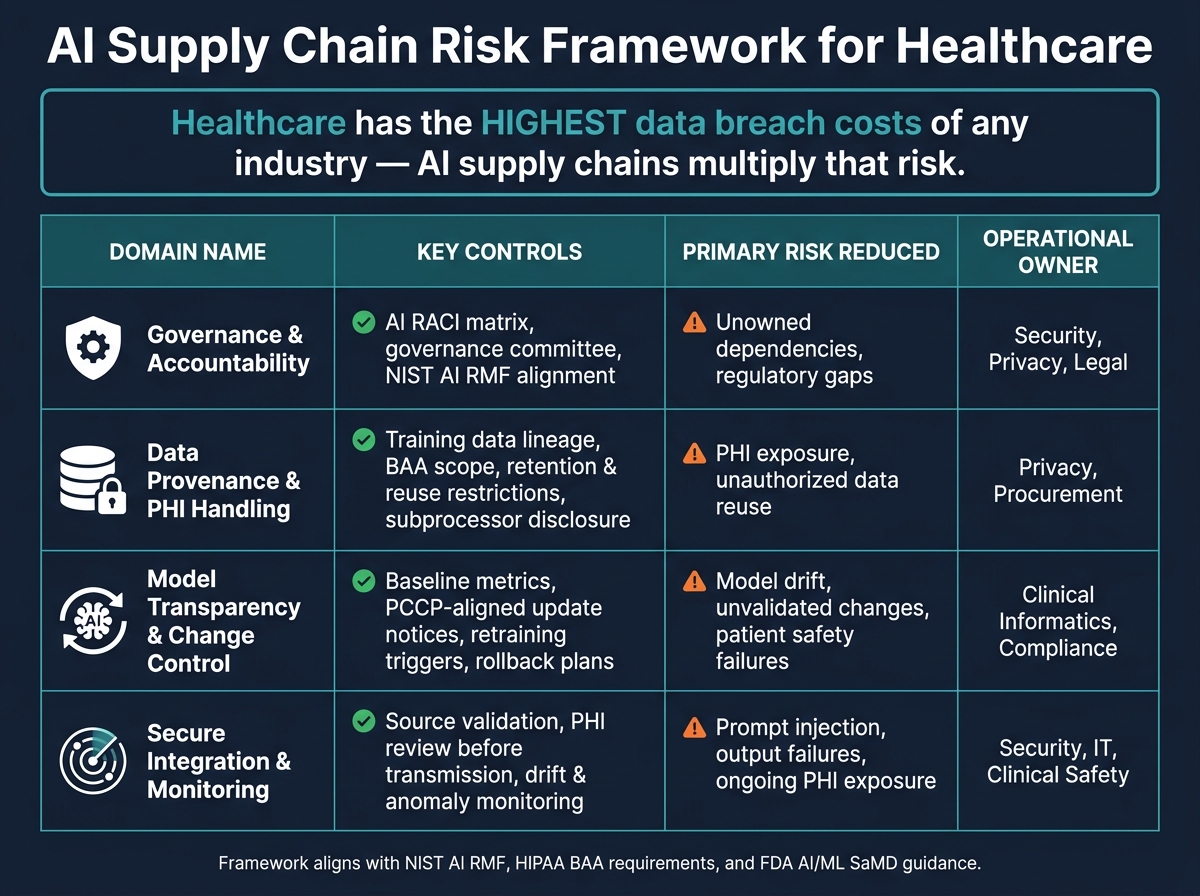
AI Supply Chain Risk Framework for Healthcare: 4 Key Domains
These risks call for an AI-specific framework built around how models are trained, connected, and watched over time. The goal is simple: turn broad AI risk into clear governance steps, contract terms, and monitoring controls.
Governance, accountability, and AI vendor oversight
Start with ownership. Hidden dependencies become a problem fast when no one is clearly in charge.
Set named owners through an AI RACI matrix across security, privacy, legal, procurement, clinical informatics, IT, and compliance. Procurement and legal should own contract language for AI transparency, subcontractor disclosure, and liability. Security should own API controls, logging review, and incident response. Privacy should own PHI handling, BAA scope, and data use restrictions. Clinical informatics should own output validation and patient safety escalation paths. Compliance should own regulatory alignment, including HIPAA and, where it applies, FDA AI/ML SaMD expectations.
An AI governance committee can coordinate reviews, exceptions, and escalation. Tying internal oversight to the NIST AI Risk Management Framework (AI RMF) gives teams a shared way to talk about risk and a solid baseline when regulators or auditors ask how AI vendors are managed. [2][4]
Data provenance, PHI handling, model transparency, and change control
Next, document what the model was built on and what it can do with PHI. Vendors should document training-data lineage, de-identification methods, evaluation data, retention periods, retraining triggers, and any customer-data use for training or fine-tuning. That should also include documentation showing how well the training data matches the intended clinical population and whether PHI was used or could be inferred. [8][9][11][14]
PHI handling needs tighter contract language for AI vendors than for standard software vendors. AI services can process PHI through prompts, logs, retrieval pipelines, model-improvement workflows, and subcontracted infrastructure. Business associate agreements should cover four areas:
- retention: how long prompts and outputs are stored
- reuse: whether PHI may be used for model training or improvement
- storage: where data lives and whether it is de-identified
- subprocessors: which third parties are allowed to access it
If a vendor's default settings go past your privacy rules, the contract should block that in plain language. [8][10][12][13]
Model drift also needs direct attention in change control. The FDA's AI/ML SaMD guidance introduces Predetermined Change Control Plans (PCCPs) - pre-approved procedures that define how a model can be updated without requiring a full regulatory submission each time. [15][16][17] In practice, the PCCP idea works well as a template: define baseline metrics, retraining triggers, advance notice, and rollback steps.
Secure integration, output validation, and continuous monitoring
Then control how AI enters your environment and how it affects decisions. Integration paths matter just as much as model behavior.
Prompt injection and output reliability risk both show up at the integration layer. RAG pipelines need source validation so injected or manipulated content does not reach clinical outputs. Prompts sent to external model APIs should also be reviewed for PHI before transmission.
Review intensity should match the use case. Administrative summarization may need lighter review. Triage, coding, diagnosis, and coverage decisions need stronger human approval. Any AI-generated recommendation that could change diagnosis, treatment, discharge, or coverage decisions should be approved by a trained reviewer before it affects care - no autonomous decisions without human approval. [9][11]
After go-live, continuous monitoring closes the loop. FDA guidance describes this as a total product lifecycle approach, built on ongoing monitoring, change validation, and incident reporting when performance shifts affect patient safety. HSCC guidance treats model drift as a risk that needs constant attention, not a one-time validation task. [1][15][16][17] Monitoring should cover drift, output anomalies, bias indicators, PHI exposure events, and any AI-related incidents.
The table below sums up the framework across its four domains:
| Framework Domain | Key Controls | Primary Risk Reduced | Operational Owner |
|---|---|---|---|
| Governance & Accountability | AI RACI matrix, governance committee, NIST AI RMF alignment | Unowned dependencies, regulatory gaps | Security, Privacy, Legal |
| Data Provenance & PHI Handling | Training data lineage, BAA scope, retention and reuse restrictions, subprocessor disclosure | PHI exposure, unauthorized data reuse | Privacy, Procurement |
| Model Transparency & Change Control | Baseline metrics, PCCP-aligned update notices, retraining triggers, rollback plans | Model drift, unvalidated changes, patient safety failures | Clinical Informatics, Compliance |
| Secure Integration & Monitoring | Source validation, PHI review before transmission, drift and anomaly monitoring | Prompt injection, output failures, ongoing PHI exposure | Security, IT, Clinical Safety |
Use this framework as the checklist for vendor due diligence, contract review, and ongoing oversight.
How to apply the framework in vendor assessments, contracts, and ongoing oversight
Use the framework in three places: vendor review, contract language, and day-to-day oversight.
AI-specific due diligence questions and evidence requests
Before you buy, use AI-specific due diligence to check model lineage, PHI flows, subcontractors, validation, and monitoring. The goal is simple: get proof, not promises.
Ask vendors for concrete evidence across three combined areas:
- Model documentation and validation: Model cards that show the architecture, foundation model provider, training objectives, known limits, and version history. Also ask for benchmark results on clinically relevant tasks, documented failure modes, and human-in-the-loop review procedures.
- Training data provenance and PHI flows: Written disclosure of data sources, de-identification methods, and whether PHI was used in training or fine-tuning. Ask for visual maps that show where PHI enters, how it moves through the system, and where it exits, including encryption, access boundaries, and data segregation.
- Subprocessor inventory and incident response: A full list of cloud providers, foundation model APIs, labeling vendors, and plug-ins. Also request documented alert thresholds, rollback procedures, logs for prompts, outputs, and user IDs, plus incident escalation timelines.
If a vendor can't provide these artifacts, treat that gap as a risk finding.
To compare vendors in a repeatable way, turn these requests into scoring templates with ratings for governance, transparency, monitoring, and response. That gives you a side-by-side view using the same yardstick each time.
Contract terms that reduce AI supply chain risk
The framework only works if the contract backs it up. Standard BAA language was built for data storage and transmission, not for AI systems that handle PHI through prompts and model-improvement workflows. Contracts need to deal with that head-on.
Four clauses matter most.
Data use restrictions in the BAA and DPA should bar vendors from using customer PHI to train or fine-tune any general or cross-customer model unless you approve it in writing.
Model change notification in the MSA should require at least 30 days' advance notice before a major model update. That notice should include expected impacts and give the healthcare organization a chance to test changes in a non-production environment before launch.
Subprocessor approval should require prior written consent before the vendor adds or changes any foundation model provider, cloud infrastructure partner, or critical API. It should also include flow-down obligations so those subprocessors meet the same security and compliance standards.
Retention and deletion commitments should cover prompts, outputs, logs, embeddings, and any derived artifacts. Those terms should spell out deletion timelines both on request and when the contract ends.
For incident response, require notice within 72 hours of discovering a breach or material AI incident. Vendor cooperation language should also make clear that the vendor must assist in any investigation where an AI recommendation contributed to an adverse event.
Once the contract sets the rules, use a shared workflow to track evidence, exceptions, and remediation.
Operationalizing AI governance with Censinet RiskOps™ and Censinet AI
Censinet RiskOps™ acts as the central system where AI vendor assessments, risk artifacts, and governance committee workflows sit in one place. AI-specific questionnaires can be deployed right in the platform, and completed assessments - model documentation, data flow diagrams, validation reports, and contracts - can be stored and tracked there. That makes it easier for security, privacy, legal, and clinical teams to get what they need without digging through scattered files.
Censinet AI™ speeds up the work inside that system. It reads vendor-submitted documents and maps the relevant details to standardized assessment questions. It also surfaces fourth-party exposures that vendors may not have flagged directly and drafts risk summary reports based on the full assessment record.
Most important, Censinet AI uses a human-in-the-loop model. Automation handles evidence validation and mitigation planning, but risk teams stay in control through configurable rules and review steps. Final decisions stay with the people accountable for them.
Conclusion: what healthcare leaders should do differently now
AI supply chains aren't just more complex software supply chains. They bring a different set of risks. Models drift. Dependencies shift. Training data is often opaque. And PHI can pass through prompts and logs in ways that standard controls may not catch. That's why the framework above puts so much weight on provenance, change control, and continuous monitoring.
The money at stake is huge: healthcare has the highest breach costs of any industry. An AI vendor failure tied to an unmonitored model update or an opaque subprocessor isn't just a compliance problem. It's also a patient-safety event.
AI vendor risk needs to be handled as an ongoing safety, privacy, and compliance function. The controls that matter most - data provenance, subprocessor visibility, output validation, and model change notification - only do their job if teams maintain them across the full life of the vendor relationship, not just during contract signing.
The next step is operational, not theoretical. Healthcare leaders should:
- Build an AI vendor inventory
- Require AI-specific due diligence
- Update contract terms
- Monitor vendors continuously with clear ownership
Treat AI vendor management as an ongoing patient-safety and regulatory duty, not a one-time IT review. Healthcare leaders that run AI vendor oversight as a continuous risk process will be in a better position to protect patients, PHI, and compliance.
FAQs
How is AI vendor risk different from software vendor risk?
AI vendor risk isn’t the same as software vendor risk.
With standard software, reviews are often point-in-time. You assess the product, check security and compliance, and move on unless something major changes.
AI works differently. These systems are dynamic, often hard to see inside, and built on multi-layered supply chains. That means risk doesn’t sit still. It can shift as models drift, performance changes, or outside dependencies change behind the scenes.
A few things make AI vendor risk stand apart:
- Limited model transparency: It’s not always clear how a model works, why it gave a certain output, or what changed from one version to the next.
- Hidden upstream providers: Many AI vendors rely on other parties for cloud infrastructure, data sources, and foundation models. Those upstream links can add risk that isn’t obvious at first glance.
- Higher stakes: In healthcare, the impact can hit patient safety, clinical workflows, and PHI - not just system uptime or general IT performance.
That’s why AI needs ongoing governance, not a one-and-done review. The job isn’t just checking whether the vendor looks good on paper. It’s also watching how the system behaves over time and how its dependencies shift in the background.
What should we ask AI vendors about PHI?
Go beyond standard software questionnaires. Ask for a signed Business Associate Agreement (BAA) that clearly says patient data can't be used for model training or fine-tuning unless you say yes.
Then get specific. Ask:
- What PHI goes into the model
- Where that data is stored
- When it is deleted from inference logs and training pipelines
- Which fourth parties may be able to access it
- Whether you have audit rights to check data governance
This is where a lot of teams stop too early. A vendor may say they’re HIPAA-ready, but that doesn’t tell you much on its own. You need plain answers about how data moves, who can touch it, and how long it sticks around.
Who should own AI vendor oversight in healthcare?
AI vendor oversight should sit with a multidisciplinary governance committee. In a healthcare setting, that means bringing the right people into the room from the start: clinical leadership, IT and informatics, cybersecurity, legal, compliance, privacy, procurement, and operations.
That setup matters because AI decisions don't live in one lane. A vendor might look fine from a procurement angle, for example, but create headaches for privacy, security, or clinical use.
For accountability, use a RACI matrix to spell out who makes decisions across the full AI lifecycle, from procurement through decommissioning. This keeps decision rights clear and cuts down on the all-too-common “I thought someone else owned that” problem.
A senior executive who reports to the CEO should coordinate the work. Then each function should own its part of the process.
